
The ventilation perfusion ratio is a key idea in lung care. It tells you how well air reaches the alveoli compared to blood flow there. This article explains what the ratio means, how to read results, and why it matters for patients and clinicians.
What is the ventilation perfusion ratio?
The ventilation perfusion ratio, often written V/Q, compares airflow to blood flow in the lung. A balanced V/Q means oxygen moves into blood and carbon dioxide leaves efficiently. When the ratio shifts, gas exchange becomes less efficient and the body can become hypoxic.
It helps to start with simple definitions. The phrase definition of ventilation tells us ventilation is the movement of air into and out of the lungs. For a quick clinical note, you may also see the term ventilation medical definition used in reports or teaching. Both point to the same idea: air reaching alveoli.
V/Q is not a single number for the whole lung. Different lung zones have different V/Q ratios. The concept of ventilation perfusion coupling describes how the body matches airflow to blood flow. Good coupling keeps oxygen and carbon dioxide levels stable. Poor coupling creates areas where blood is not well oxygenated or areas where air does not meet perfused blood.
Keeping these basics in mind helps you read clinical tests. The V/Q ratio guides diagnosis and treatment. It explains why some patients respond to oxygen and others need more advanced support.
Normal values and regional differences
Normal average V/Q for the whole lung is around 0.8 to 1.0. This means blood flow slightly exceeds ventilation at rest. That average hides important regional differences in the lung. Gravity, body position, and lung shape change ventilation and perfusion from top to bottom of the lung.
In an upright person, the top of the lung has higher V/Q. Air reaches the top easily, but less blood flows there. The base of the lung has lower V/Q because it gets more blood but slightly less air per unit volume. These natural differences are normal and well tolerated in healthy people.
Understanding these patterns matters when you interpret tests. A single global V/Q number may mask small but important mismatches. Clinicians often focus on regional changes when conditions like embolism or consolidation are suspected. That helps explain symptoms and direct treatment choices.
Types of V/Q mismatch
When V/Q is out of range, it creates clinical problems. There are a few key patterns to learn. Each pattern affects oxygenation and carbon dioxide removal in different ways.
Below is a clear list of the common types of V/Q mismatch and what they mean. Read the short descriptions to see how each type presents and how it affects gas exchange.
- Shunt (V/Q = 0): Blood flows past alveoli that are not ventilated. This occurs with airway blockage or lung consolidation. Oxygen therapy often has limited effect on pure shunt.
- Low V/Q: Ventilation is reduced relative to perfusion. This is common in COPD and asthma. Oxygen helps but underlying ventilation needs attention.
- High V/Q: Ventilation exceeds perfusion in a lung region. This happens when blood flow drops, for example with pulmonary embolism. Areas with high V/Q act like wasted ventilation.
- Dead space (very high V/Q): Air reaches alveoli but no blood flow occurs. The air is wasted for gas exchange. Mechanical ventilation and monitoring help manage dead space issues.
Knowing these types helps clinicians choose tests and treatments. For example, shunt and low V/Q often respond differently to oxygen therapy. High V/Q and dead space suggest a vascular problem that may need imaging or anticoagulation.
How V/Q is measured and reported
There are several ways clinicians assess V/Q status. No single test gives a full picture. Reviewing blood gases, imaging, and bedside measures together gives the best view. Each test has strengths and limits.
Common tests include arterial blood gas measurements, V/Q nuclear scans, chest CT angiography, pulse oximetry, and capnography. Arterial blood gas shows oxygen and carbon dioxide levels and helps estimate the alveolar-arterial gradient. A V/Q scan maps regional ventilation and perfusion. CT angiography directly images clots in the pulmonary arteries.
It is useful to know the difference between some terms. For example, compare ventilation vs respiration. Ventilation is airflow; respiration refers to gas exchange at the tissues. This distinction clarifies test results and therapy choices. In practice, clinicians use multiple data points to interpret V/Q mismatch.
Reports may present a qualitative description or a numerical V/Q ratio. For teaching and quick decisions, recognizing patterns on imaging or labs matters more than a single ratio. The clinical context, such as history and exam, guides which test to order and how to read it.
Common clinical scenarios
The V/Q concept applies in many conditions. Knowing typical patterns helps you interpret tests quickly. Here we cover four frequent scenarios and what to expect for V/Q changes.
In each scenario you will see a repeat pattern of symptoms and test results. Learning these patterns helps with early recognition and faster treatment. Repeat study of scenarios makes interpretation easier in practice.
After reading the short summaries below, you should be able to link a clinical picture to a likely V/Q issue. That will guide the next steps in care and testing.
Pulmonary embolism
Pulmonary embolism commonly causes areas of high V/Q or dead space. A clot blocks blood flow but leaves ventilation intact. Patients may have sudden shortness of breath, chest pain, and low oxygen levels with relatively normal lung exam in some cases.
On testing, you may see a normal chest x-ray, low oxygen on arterial blood gas, and a mismatch on V/Q scan where ventilation is present but perfusion is absent. CT pulmonary angiography often confirms the clot and maps its size and location.
Recognizing this pattern is urgent. Treatment usually targets the clot and supports oxygen delivery. Quick interpretation can be life saving.
COPD and chronic lung disease
Chronic obstructive lung disease often causes low V/Q areas. Narrowed airways and mucus reduce ventilation in parts of the lung while perfusion remains. Patients have long-term breathlessness and can worsen with infection or flare.
In COPD exacerbations, oxygen levels fall and carbon dioxide may rise depending on the severity and chronic compensation. V/Q scans show broad regions with reduced ventilation. Treatment focuses on bronchodilators, steroids, oxygen when needed, and careful ventilatory support if required.
Understanding the low V/Q pattern helps avoid overuse of oxygen in some cases and guides ventilator settings when invasive support is needed.
Pneumonia and consolidation
Lobar pneumonia or alveolar consolidation causes shunt physiology in the affected region. Air cannot reach alveoli, but blood still flows through the area. This creates poorly oxygenated blood mixing with well oxygenated blood and lowers the overall oxygen level.
Patients often have fever, productive cough, and crackles on exam. Chest imaging shows focal consolidation. Oxygen therapy commonly improves saturation because increasing inspired oxygen raises the oxygen content of ventilated lung units.
Recognizing shunt physiology guides early antibiotic treatment and supportive care. It also explains why oxygen usually helps these patients more than cases with large shunt fractions that are resistant to oxygen.
ARDS and critical illness
Acute respiratory distress syndrome creates widespread low V/Q and shunt. The alveoli become flooded or collapse across large lung areas. Patients are severely hypoxic and often require mechanical ventilation in an intensive care setting.
In ARDS, V/Q heterogeneity is marked. Management focuses on lung protective strategies, positional therapy, and careful control of oxygen and ventilation. Strategies aim to recruit collapsed lung units and reduce further injury from high pressures.
Interpreting V/Q patterns in ARDS guides choices such as using positive end-expiratory pressure, proning, and selecting ventilator modes tailored to lung mechanics.
Management and implications for ventilation
Interpreting V/Q helps decide on therapy. Some mismatches respond well to oxygen. Others need targeted treatment like anticoagulation or drainage. Mechanical ventilation requires a clear plan that matches the V/Q problem.
Below is a practical list of management steps tied to V/Q patterns. Read the lead-in to know when each option is most useful. These steps are a general guide and must be adapted to the patient and local protocols.
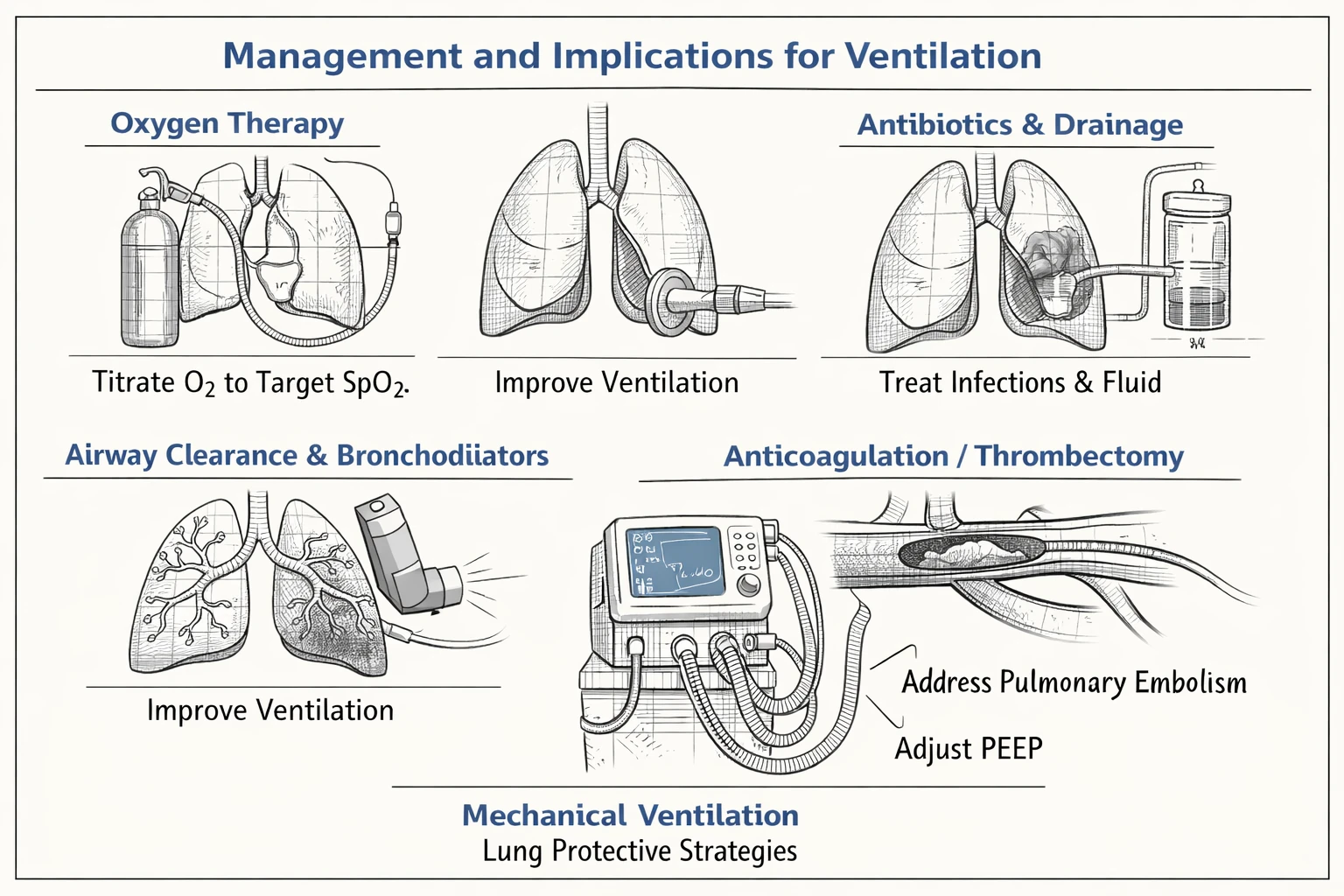
- Oxygen therapy: Useful for low V/Q and some shunt situations. Titrate to target oxygen saturation while avoiding oxygen toxicity in chronic CO2 retainers.
- Airway clearance and bronchodilators: Help in obstructive disease to improve ventilation and raise V/Q in affected units.
- Antibiotics and drainage: Treat consolidation and infected fluid that cause shunt physiology.
- Anticoagulation or thrombectomy: Indicated for pulmonary embolism creating high V/Q or dead space.
- Mechanical ventilation strategies: Use lung protective volumes, adjust PEEP to recruit collapsed units, and select appropriate ventilator modes for the patient's mechanics and drive.
Choosing ventilator settings requires thought about the difference between ventilation and gas exchange. The clinical phrase ventilation vs respiration reminds us that moving air does not always fix gas exchange. Some ventilator modes improve ventilation but may not fix perfusion mismatch. Matching settings to the specific V/Q issue improves outcomes.
When using mechanical ventilation, monitor blood gases and lung mechanics closely. Adjust PEEP to improve oxygenation while watching for overdistension. Consider proning to redistribute perfusion and improve ventilation perfusion coupling in severe cases. These interventions require teamwork and repeated reassessment.
Key Takeaways
The ventilation perfusion ratio is central to understanding oxygenation problems. It links airflow to blood flow and explains many clinical patterns. Keep the basic types in mind: shunt, low V/Q, high V/Q, and dead space.
Use multiple tests to interpret V/Q. Blood gases, imaging, and bedside measures together give the best picture. Remember simple phrases like definition of ventilation and ventilation medical definition to keep terms clear when teaching or reading reports.
In practice, link the likely V/Q pattern to targeted treatment. Oxygen helps many low V/Q and some shunt cases. Vascular problems need imaging and possible anticoagulation. Mechanical ventilation and the right ventilator modes can improve outcomes when used with an understanding of ventilation perfusion coupling.
With frequent practice, reading V/Q issues becomes faster and more accurate. Keep learning through cases, and use this guide as a clear map to interpret results and choose next steps with confidence.